To be very clear out of the gate, we are neither anti-statin nor pro-statin. We are pro-information.
June is Men’s Heart Health Month. We are passionate about men’s and women’s heart health. So, let’s talk High Cholesterol and Statins.
One of the most common questions we hear in the office is: “I have high cholesterol. Do I need a statin?” And other times the question is the opposite: “My cholesterol is normal, so my risk of heart disease or heart attack/stroke is low… right?”

Neither answer is that simple. Over the years, we’ve seen patients with “perfect” cholesterol suffer heart attacks, and we’ve seen patients with elevated cholesterol who have little evidence of cardiovascular disease. That’s because heart disease is far more complicated than a cholesterol and LDL numbers.
Many people think cholesterol itself causes heart disease. In reality, cholesterol is a normal and necessary part of human physiology. Cholesterol is used to make hormones, cell membranes, vitamin D, bile acids, and many other critical substances.
The more information we have about an individual’s cardiovascular risk, the more personalized and appropriate the recommendation becomes. This is one of the reasons we are passionate about advanced cardiovascular testing rather than relying solely on a standard lipid panel. When we’re deciding whether lifestyle changes are enough, whether medication should be considered, or whether someone needs more aggressive intervention, we look at a much bigger picture.
Lab markers are great for giving a PIECE of information; however, we look for WHO the person is behind the lab result. How old are they? What does their family history look like? Do they have a parent or sibling who had a heart attack (if so, at what age, and what was their lifestyle and other health issues)? What is this person’s blood pressure (without medication)? Do they exercise regularly? Are they insulin resistant? What does their A1c (3 month blood sugar) look like? How are they sleeping? Do they have chronic inflammation, autoimmune disease, high stress levels, or excess visceral fat?
For women, are they in perimenopause or menopause and experiencing the metabolic changes that often occur with declining estrogen levels?
We know that where someone lives, their access to healthy food, their finances (to afford healthy food, gym memberships or sneakers that aren’t worn out), socioeconomic environment, medications, stress levels, and activity patterns all influence cardiovascular risk. A cholesterol number by itself cannot answer those questions.
Why The Standard Lipid Panel Doesn’t Tell the Whole Story
Most annual physicals include a standard lipid panel that measures Total Cholesterol, LDL, HDL, Triglycerides (and often a Chol/HDL ratio). These standard panels tell us how much cholesterol is being carried. These markers are helpful, but they don’t tell us: How many cholesterol particles are circulating, whether those particles are large or small, whether inflammation is damaging blood vessels, whether plaque is actively developing, whether genetics are increasing risk or whether insulin resistance is contributing to cardiovascular disease.
Advanced testing such as a Cardio IQ Advanced Lipid Panel helps us understand how that cholesterol is being carried, whether the particles are likely to contribute to plaque formation, and whether inflammation is increasing cardiovascular risk. And for most patients, these advanced panels are easily accessible labs and often covered by insurance (of course deductibles all vary).
Normal vs. Optimal: They Are Not Always the Same
One of the biggest sources of confusion in medicine is the difference between a laboratory reference range and an optimal range. Most people assume that if a result falls within the laboratory’s “normal” range, everything is fine. Unfortunately, that’s not always the case.
Only about 12% of American adults are considered metabolically healthy (88% are not). Nearly 74% of U.S. adults are overweight or obese, approximately 38% have prediabetes, an estimated 70-88% have some degree of metabolic dysfunction or insulin resistance, only 30% of adults achieve recommended physical activity levels, roughly one-third of adults report getting less than the recommended 7 hours of sleep, and 6 in 10 Americans have at least one chronic disease while 4 in 10 have two or more chronic conditions.
Laboratory reference ranges are primarily designed to help identify and diagnose disease. In many cases, they are based on statistical averages from the general population rather than levels associated with optimal health, longevity, or disease prevention. When these are the populations used to establish many laboratory reference ranges, “normal” may simply reflect what is common, not necessarily what is optimal for long-term health and disease prevention. As a result, a “normal” laboratory value may simply mean you look similar to everyone else being tested and not necessarily that you are in the healthiest range possible.
In traditional medicine, many laboratory tests are used to determine whether disease is present and whether treatment is necessary. In functional and preventive medicine, we often ask a different question: Is this marker moving in a direction that supports long-term health, or is it moving toward disease?
For example, an hs-CRP of 2.8 mg/L may technically be considered “normal” by laboratory standards, but it still suggests a level of inflammation associated with increased cardiovascular risk and suspicious for systemic inflammation. Similarly, a fasting insulin of 18 uIU/mL is considered “normal” and won’t trigger a diagnosis, but it does increase suspicion for insulin resistance years before blood sugar levels become abnormal enough to be labeled prediabetes or diabetes.
In functional and preventative medicine, we also pay close attention to trends. A cholesterol level, ApoB, fasting insulin, inflammatory marker, or calcium score does not exist in isolation. Understanding whether a marker is improving, worsening, or remaining stable over time often provides more meaningful information than a single snapshot.
Our bodies, environment, diet, stress, hormones and bodies are forever in motion. This is why we repeat testing after implementing nutrition, exercise, hormone, supplement, sleep, or lifestyle interventions. We want to know whether the body is moving toward greater health or toward greater disease risk.
Menopause, Cholesterol, and Cardiovascular Risk
One important factor that is often overlooked when evaluating cholesterol is menopause. Many women are surprised when cholesterol levels suddenly worsen during their 40s and 50s despite maintaining the same nutrition and exercise habits they have followed for years. As estrogen levels decline during perimenopause and menopause, many women experience an increase in total cholesterol and LDL cholesterol even when their weight, diet, and exercise habits have not changed. Studies suggest LDL cholesterol commonly rises by approximately 10-20% during the menopausal transition, which can translate to increases of 15-20 mg/dL or more in many women.
At the same time, LDL particles often become smaller, denser, and more atherogenic (more likely to contribute to plaque formation), while inflammation and insulin resistance may also increase. It’s not just that cholesterol numbers rise, the cardiovascular “environment” often becomes more inflammatory and metabolically unfavorable.
When appropriate for the woman, hormone replacement therapy (HRT) – now called Menopause replacement therapy (MRT) such as transdermal estradiol started during the perimenopausal or early postmenopausal years can often help mitigate or reduce some of these shifts. Research has demonstrated improvements in LDL cholesterol, total cholesterol, insulin sensitivity, vascular function, and several markers of cardiometabolic health in women who initiate MRT within the appropriate treatment window.
This does not mean MRT should be used solely as a cholesterol medication. However, when evaluating cardiovascular risk in women, menopausal status and hormone health deserve a seat at the table alongside cholesterol numbers, blood pressure, blood sugar, inflammation markers, family history, and lifestyle habits.
Why We Frequently Order Cardio IQ Testing
The Cardio IQ Advanced Lipid Panel allows us to look beyond cholesterol levels and evaluate cholesterol particle number, particle size, inflammation, and inherited cardiovascular risk factors. Many people who develop cardiovascular disease have cholesterol levels that would not have raised concern on a standard lipid panel.
ApoB: One of the Most Important Numbers You’ve Probably Never Heard Of
One of the most important markers we review is Apolipoprotein B (ApoB).
Think of ApoB as a count of the actual particles capable of entering the artery wall and contributing to plaque formation. LDL cholesterol tells us how much cholesterol is being carried. ApoB tells us how many vehicles are carrying it. We don’t want traffic on our way to work, nor do we want it in our vessels. Two people can have the same LDL cholesterol level but dramatically different ApoB levels and therefore very different cardiovascular risk.
LDL Fractionation and Particle Size
LDL fractionation is a way to look at the behavior of the LDL. Just like humans, not all LDL particles behave the same way. Some LDL particles are large and buoyant. They go through the vessels like the kind person who opens doors for people, helps people with groceries and lets them go in front of them in traffic. Smaller, denser LDL particles are more like the jerks who cut us off in traffic, let the door slam in your face or break everything they touch. They’re more aggressive, toxic and more likely to penetrate the artery wall, become oxidized, and contribute to plaque formation.
This is why LDL fractionation testing can be so valuable. Rather than simply asking how much LDL cholesterol exists, we’re asking what type of LDL particles are present and whether those particles are likely to contribute to cardiovascular disease.
Homocysteine: A Heart Risk Marker Most Have Never Heard Of or Tested:
Homocysteine is an amino acid produced during normal metabolism. When levels become elevated, it can damage the lining of blood vessels, increase oxidative stress, promote inflammation, and contribute to plaque instability. Two people can have the exact same cholesterol level, yet very different cardiovascular risk profiles depending on what is happening beneath the surface. While many conventional lipid panels never include homocysteine testing, it can provide valuable insight into cardiovascular risk, especially in patients with a family history of heart disease, stroke, dementia, or unexplained vascular disease.
Elevated homocysteine has been associated with:
- Increased risk of heart attack and stroke
- Endothelial dysfunction (damage to the inner lining of blood vessels)
- Increased blood clotting tendency
- Cognitive decline and dementia
- Poor methylation and detoxification capacity
Common causes of elevated homocysteine include low B vitamins such as folate, B12 and B6 often caused by MTHFR genetic variants. Chronic inflammation caused by smoking, excessive alcohol intake and kidney dysfunction can also drive elevated homocysteine.
Lipoprotein(a): A Genetic Risk Factor Most People Have Never Tested
Lp(a) is largely genetic and is associated with increased risk of heart attack, stroke, and aortic valve disease. Unlike many cardiovascular markers, Lp(a) is minimally affected by diet and exercise. This is why we believe everyone should have Lp(a) measured at least once during adulthood.
If elevated, it may help explain why cardiovascular disease runs strongly in a family despite healthy lifestyle habits.
One important caveat, for women, is that while Lp(a) is generally considered a “once-in-a-lifetime” test because levels tend to remain relatively stable whether they are high or low, menopause can be an outlier with this one time test rule. As estrogen levels decline during the menopausal transition and inflammation rises, Lp(a) levels may increase, contributing to the rise in cardiovascular risk seen after menopause. Conversely, MRT, particularly estrogen therapy in appropriate candidates, has been shown to reduce Lp(a) levels in many women. For this reason, women who had Lp(a) measured years before menopause may benefit from repeat testing during the menopausal transition or after menopause, especially if cardiovascular risk factors have changed or they’re being told to start a statin.
Heart Disease Is Also an Inflammation Problem
For years, cholesterol was viewed as the primary driver of heart disease. Today we understand that inflammation plays a major role as well. The Cardio IQ panel includes hs-CRP (high-sensitivity C-reactive protein), which measures systemic inflammation throughout the body, and Lp-PLA2, which evaluates inflammation occurring within blood vessel walls.
When inflammatory markers are elevated, we start asking additional questions: Is there insulin resistance? Poor sleep? An autoimmune condition? Periodontal (teeth/mouth/gum) disease? Excess visceral fat? Chronic stress? Gut dysfunction or imbalances?
An Inflammation Marker We Often Add: Oxidized LDL
As stated earlier in the blog, cholesterol is not inherently ‘bad’, nor is LDL. The problem occurs when LDL particles become damaged (oxidized). Oxidized LDL refers to LDL cholesterol that has been altered by oxidative stress and inflammation. Once oxidized, LDL becomes much more likely to enter the artery wall, trigger inflammation, and contribute to plaque formation. It is entirely possible for someone to have a relatively normal LDL cholesterol level but elevated oxidized LDL and increased cardiovascular risk.
Think of LDL as a delivery truck. Oxidized LDL is the delivery truck after it has been damaged, leaking gas and antifreeze, without breaks causing accidents along the highway.
This is why functional and preventative medicine doesn’t focus solely on a traditional lipid panel, but what is happening driving the inflammatory dynamic, insulin resistance, smoking, poor sleep, nutrient deficiencies, environmental exposures, and metabolic health.
When evaluating cardiovascular risk, we frequently look beyond the laboratory “normal” range and consider what research suggests may be associated with lower cardiovascular risk, better metabolic health, healthier aging, and improved long-term outcomes.
Here’s a reference chart for you to peek at your labs and see where you sit:
“Normal” or “Optimal”?
| Total Cholesterol | <200 mg/dL | Context Matters |
| LDL-C | <100 mg/dL | Individualized |
| HDL-C | >40 men / >50 women | >60 mg/dL |
| Triglycerides | <150 mg/dL | <80 mg/dL |
| hs-CRP | <3.0 mg/L | <1.0 mg/L |
| Fasting Insulin * | 2–25 μIU/mL | <8 μIU/mL |
| HbA1c | <5.7% | <5.3% |
| ApoB | <90 mg/dL | <80 mg/dL |
| Lp(a) | <75 nmol/L | As Low As Possible |
| Homocysteine | 5–15 μmol/L | 6–8 μmol/L |
| HbA1c* | <5.7% | <5.3% |
| Blood Pressure* | <120/80 mmHg | <115/75 mmHg |
*Not part of the Cardio IQ panel but frequently evaluated alongside cardiovascular risk.
One of Our Favorite Tests: The Coronary Calcium Score
If there is one cardiovascular test that has changed clinical decision-making more than almost any other, it is the Coronary Artery Calcium (CAC) Scan. The CAC is a non-invasive CT scan measures calcified plaque within the coronary arteries. Optimally we want the CAC score to be zero. While a score of zero doesn’t guarantee someone will never develop heart disease, it is one of the strongest indicators that short-term cardiovascular risk is low.
We commonly consider a CAC scan in:
- Men over age 40 with risk factors
- Women over age 50 or post-menopause
- Individuals with elevated ApoB
- Individuals with elevated Lp(a)
- Strong family history of premature heart disease
- Patients unsure about statin therapy
| CAC Score | Interpretation |
| 0 | No detectable plaque |
| 1-99 | Mild plaque burden |
| 100-299 | Moderate plaque burden |
| 300-399 | Significant plaque burden |
| 400+ | Extensive plaque burden and substantially elevated risk |
ASCVD Risk Calculator and Mayo Clinic Statin Choice Decision Aids
Two of the most useful cardiovascular decision-making tools available to clinicians and patients are the ASCVD Risk Calculator and the Mayo Clinic Statin Choice Decision Aids. These tools help patients better understand their individual risk and allow for more informed discussions about treatment options. Neither of these tools are new, expensive, or difficult to access. They are freely available online and can be used by virtually any healthcare provider or patient. Yet many patients have never heard of them, and most providers are not using them for decisions making.
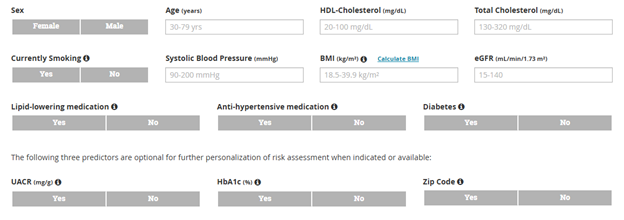
The ASCVD Risk Calculator estimates a person’s likelihood of having a heart attack or stroke over the next 10 years using factors such as age, cholesterol levels, blood pressure, smoking history, and diabetes status. And they’ve recently added additional optional data for deeper personalized risk assessment.
The Mayo Clinic Statin Choice Decision Aid takes the conversation one step further.
Rather than simply recommending a statin based on a cholesterol number, it helps estimate the potential benefit of treatment based on an individual’s overall cardiovascular risk, giving heart attack risk estimations without statin, with standard dosing and high dose statin. A medication may reduce cardiovascular risk, but the amount of benefit depends heavily on the individual’s starting risk.
For someone with established cardiovascular disease, diabetes, significant plaque burden, or multiple risk factors, the benefit may be substantial. For someone with a very low baseline risk, excellent metabolic health, and no evidence of plaque, the benefit may be much smaller. This highlights why personalized medicine matters.
However, they still don’t account for many of the factors we know influence cardiovascular disease, including lifestyle (diet, exercise, sleep, finances), ApoB, Lipoprotein(a), fasting insulin, inflammation markers, hormone status, coronary calcium scoring, and many nuances of family history.
When Might a Carotid Ultrasound Be Helpful?
A carotid artery ultrasound evaluates plaque formation within the carotid arteries of the neck. Unlike a CAC scan, it can identify both calcified and non-calcified plaque and assess arterial wall thickness.
We often consider carotid imaging when:
- There is a strong family history of stroke
- Lp(a), ApoB, Oxidized LDL, or CRP are elevated
- Elevated CAC scores
- There is concern for early vascular disease despite a CAC score of zero
A normal carotid ultrasound and a CAC score of zero can be very reassuring. Conversely, plaque identified on either study may support a more aggressive prevention strategy.
If You Take a Statin, Please Consider CoQ10
One conversation that is often overlooked is CoQ10 depletion. All statins work by inhibiting the mevalonate pathway. Unfortunately, this same pathway is involved in producing CoQ10. CoQ10 is critical for mitochondrial function (the ‘energy machines’ in all of our cells), cellular energy production, muscle function, heart function, and brain function.
For patients taking statins, we commonly recommend discussing supplementation with their healthcare provider. We recommend 200 mg daily of the Ubiquinol form, taken at the opposite time of day from the statin. Example: If the statin is taken at bedtime, take Ubiquinol in the morning. This supplementation supports mitochondrial function and reduces the risk of statin-associated muscle symptoms.
How Often Should Testing Be Repeated?
If we are implementing nutrition, exercise, supplement, hormone, or lifestyle changes, we typically repeat advanced lipid testing in approximately three to six months. This time frame allows us to evaluate whether interventions are producing meaningful improvements. Cardiovascular health is dynamic. What your labs looked like five years ago may have little relevance to what is happening today.
Beyond the Cholesterol and LDL Numbers
When it comes to cardiovascular disease, cholesterol is only one piece of a much larger story. Advanced lipid testing, inflammation markers, blood sugar regulation, blood pressure, family history, sleep quality, exercise habits, hormone status, coronary calcium scoring, and overall metabolic health all help create a more complete picture.
Sometimes a statin is absolutely the right choice. Sometimes lifestyle interventions deserve more time. Most often, the best decisions come from looking at the whole person rather than a single lab value.
Need a practitioner who look at more than cholesterol and LDL numbers? A practitioner who is passionate about looking deeper? We’re here for you and your loved ones. Contact us 4 Better Health.